Retake
P17) New-onset seizures, headache, and vomiting
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a pediatric patient with headache and vomiting.
- Review the DDx considerations in a pediatric patient with headache and vomiting.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a pediatric patient with headache and vomiting.
History
A 15-year-old boy to the pediatric emergency department following a new-onset seizure that resolved on its own. The patient also reports five weeks of worsening headaches and episodes of nausea and vomiting occurring in the morning.
Physical Exam
BP: 110/85, HR 60, RR 12, Temp 99.1F, O2 saturation 98%. Neuro: ataxic gait. Difficulty performing finger to nose testing. Dysdiadochokinesia. Disconjugate gaze with lateral eye movements. Diplopia on lateral gaze bilaterally. Bilateral papilledema on optic nerve examination.
Labs
CBC and CMP results within normal limits.
Provisional Diagnosis
Select the Dx you believe is most appropriate
This patient with new-onset progressive headache, vomiting, and acute cerebellar ataxia (ataxic gait, dysdiadochokinesia, and difficulty with finger-to-nose testing) most likely has a brain tumor in the posterior fossa. This mass lesion likely results in hydrocephalus considering the papilledema and CNVI palsy.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires urgent workup and management.
First Imaging Study
What is the first imaging study you will order?
A brain MRI with and without contrast can help identify and characterize a brain mass lesion. In this pediatric patient who is not undergoing emergent imaging and is without contraindication to MRI, CT should be avoided to minimize radiation.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
MRI with and without contrast
What ventricle is the mass located in?
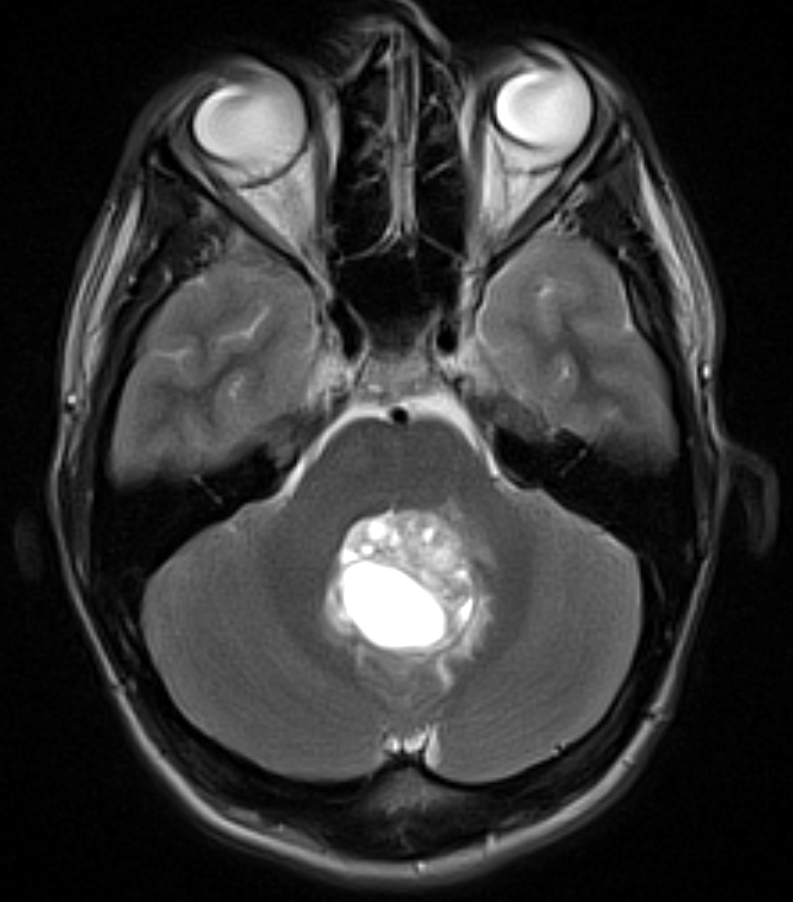
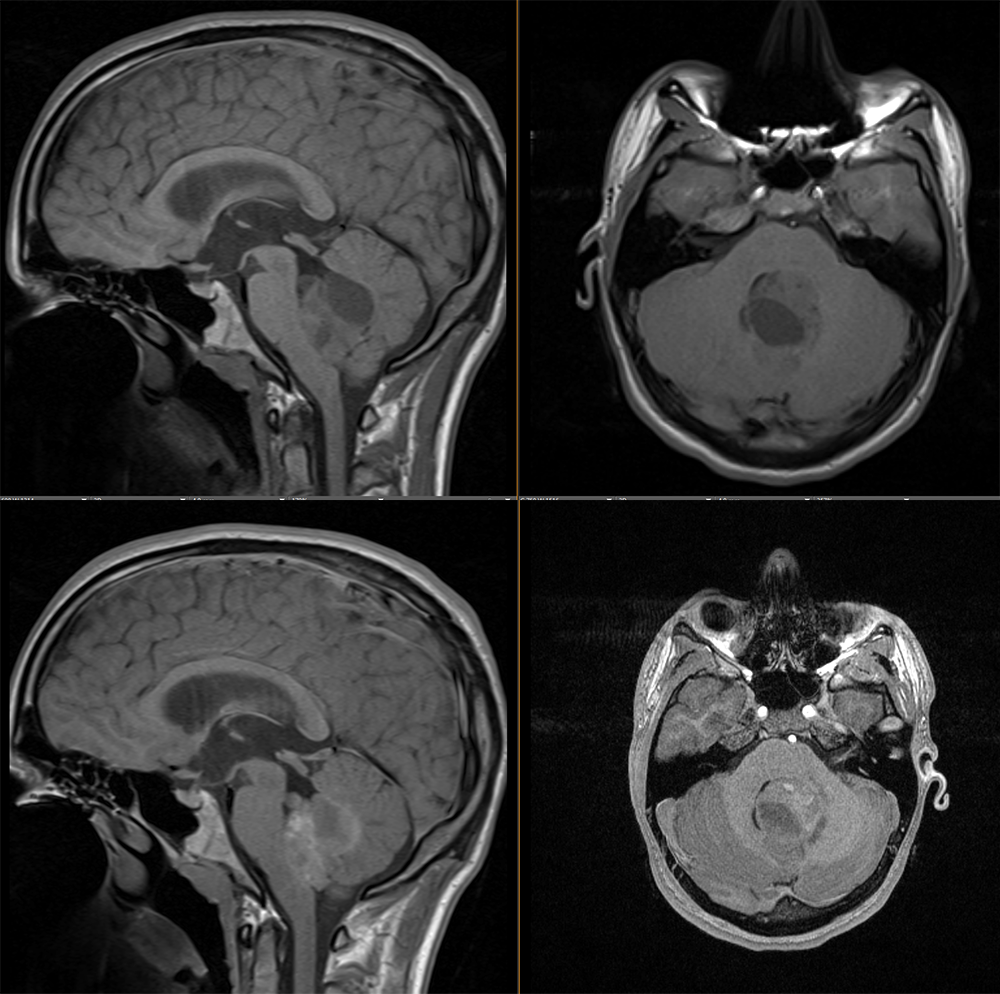
There is a fourth ventricular mass.
The lesion homogeneously enhances with IV contrast.
The solid component of the lesion demonstrates heterogeneous enhancement.
The ventricles are normal.
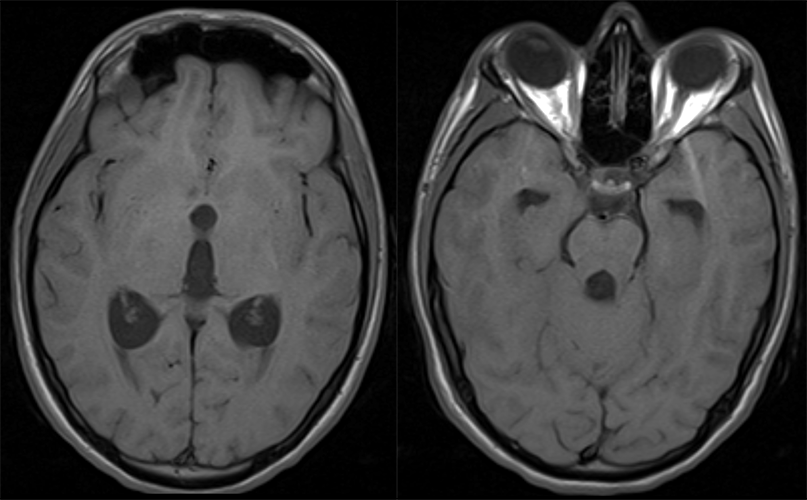
The images show that the third and fourth ventricles are abnormally dilated. Therefore, the lesion results in obstructive hydrocephalus.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No further imaging is needed.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient likely has an ependymoma. A medulloblastoma also shares similar features (patient demographic, location in 4th ventricle) but is more likely to be homogeneous.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient will require urgent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
This patient is a 15-year-old boy presenting with a posterior fossa mass lesion with resultant hydrocephalus. Pediatric neurosurgery should be urgently consulted. In the interim, the patient should be made NPO and placed on IV fluids in preparation for surgical intervention. The patient should undergo serial neurological exams. Steroids (like dexamethasone) should be started to decrease inflammation from the tumor and alleviate symptoms from the increased ICP.
Lessons Learned:
- Most pediatric brain tumors are infratentorial. The most common infratentorial brain tumor is a medulloblastoma. However, ependymomas, pilocytic astrocytomas, medulloblastomas, pinealomas, and craniopharyngiomas can also occur.
- When the diagnosis is suspected in a pediatric patient, an MRI with and without contrast should be performed to avoid radiation dosage.
- Compared to medulloblastomas, ependymomas are more likely to be heterogeneous and with coarse calcifications.
Socioeconomic Factors:
- There is a positive correlation between parental educational and income level with a risk of pediatric ependymomas.
- Increased age is associated with improved survival in children with ependymomas.
- African Americans with ependymomas have a higher risk of mortality when compared to others.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}